
Generic drugs save the U.S. healthcare system billions of dollars every year, but have you ever wondered why your pharmacist hands you a white pill instead of the colorful brand-name one? The answer lies in a scientific concept called bioequivalence, which is the absence of a significant difference in the rate and extent to which the active ingredient becomes available at the site of drug action. It is not just about having the same chemical name; it is about proving that the generic version works inside your body exactly like the original brand-name product.
The U.S. Food and Drug Administration (FDA) sets strict rules to ensure this equivalence. These rules were established by the Hatch-Waxman Act of 1984, which created a pathway for generic manufacturers to prove their drugs are safe and effective without repeating all the expensive clinical trials done for the brand-name drug. If a generic meets these bioequivalence standards, the FDA assumes it will have the same clinical effect and safety profile as the reference listed drug (RLD).
What Is Bioequivalence?
Bioequivalence is a regulatory standard defined in 21 CFR § 320.1. In simple terms, it means that when you take a generic drug, your body absorbs it at the same speed and to the same degree as the brand-name version. This does not mean the pills look the same or contain the exact same inactive ingredients (like dyes or binders). Instead, it focuses on the active moiety-the part of the drug that actually treats your condition.
To prove this, manufacturers conduct studies under similar conditions using appropriately designed trials. The goal is to create a scientifically valid bridge between the branded product and the generic one. If bioequivalence is established, the preclinical and clinical research findings from the brand-name drug apply to the generic. This saves time and money while ensuring patients receive treatment that works reliably.
How the FDA Measures Bioequivalence
The FDA evaluates bioequivalence using pharmacokinetic (PK) parameters measured in randomized crossover trials. These studies typically involve 24 to 36 healthy volunteers who take both the generic and the brand-name drug at different times. Researchers then measure how much of the drug enters the bloodstream and how fast it happens.
Two primary PK parameters are examined:
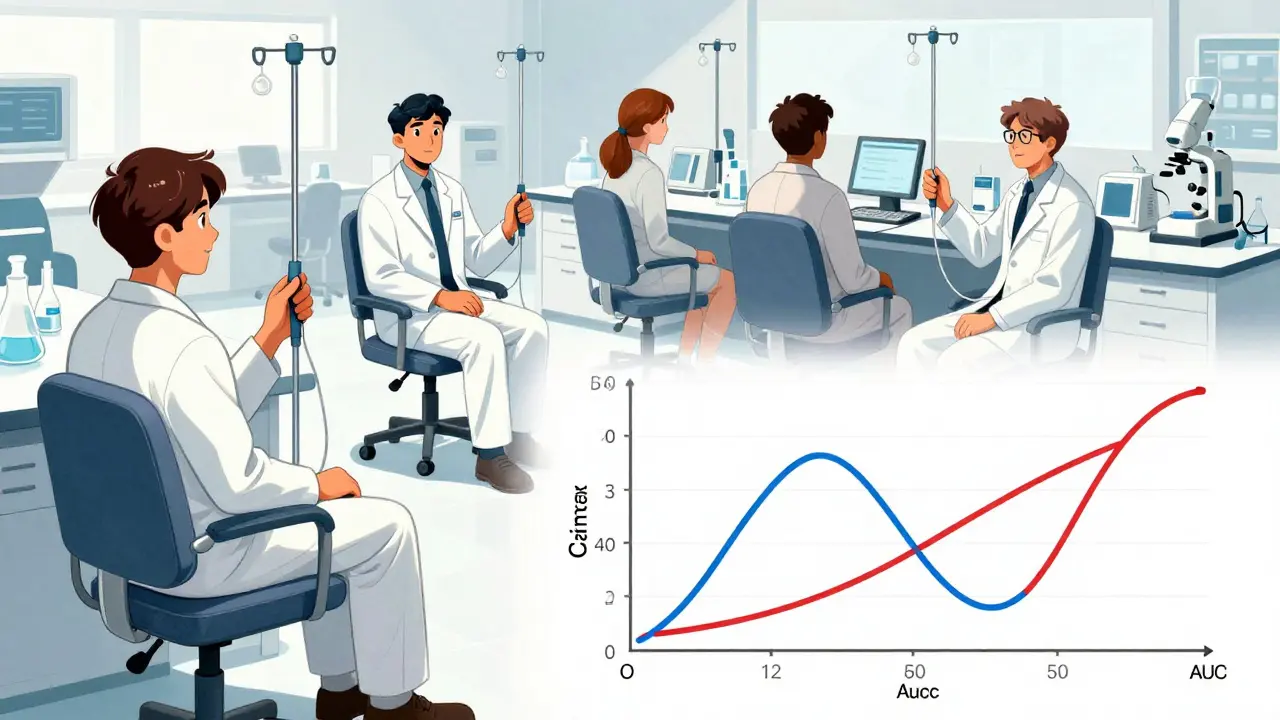
- Cmax (Peak Concentration): This measures the highest concentration of the drug in the blood after taking it. It tells us how quickly the drug starts working.
- AUC (Area Under the Curve): This represents the total amount of drug absorbed over time. There are two types: AUC(0-t), which is the area from time zero to the last measurable concentration, and AUC(0-∞), which extrapolated to infinity).
The FDA requires applicants to use the most accurate, sensitive, and reproducible approach available, as stated in 21 CFR 320.24(a). For systemic drugs intended to be absorbed into the bloodstream, in vivo testing (testing in humans) is typically required. However, for drugs acting locally, such as topical creams or inhalers, in vitro testing (testing in a lab) may suffice.
The 80-125% Rule: What It Really Means
You might have heard that generic drugs can differ from brand-name drugs by up to 20%. This is a common misconception. The FDA requires that the 90% confidence interval (CI) of the ratio of generic to reference drug must fall within the range of 80% to 125% for both Cmax and AUC parameters. This is known as the 80-125% rule.
This range applies to the pharmacokinetic parameters, not the actual amount of active ingredient in the formulation. Both the mean PK values AND the entire 90% confidence interval must fall within this range. Let’s look at an example:
If a brand-name product has an AUC of 100 units, and the generic product demonstrates an observed mean AUC of 93 with a calculated 90% CI of 84-110, this meets the bioequivalence requirement. Why? Because both the mean (93%) and the entire confidence interval (84-110%) fall within the 80-125% range. Conversely, if the upper bound of the confidence interval exceeds 125%, the drug fails bioequivalence.
| Parameter | Brand-Name Value | Generic Mean Value | 90% Confidence Interval | Result |
|---|---|---|---|---|
| AUC | 100 units | 93 units | 84 - 110% | Passes (within 80-125%) |
| AUC | 100 units | 116 units | 103 - 130% | Fails (upper bound > 125%) |
Dr. Utpal Munshi, an expert in bioequivalence studies, emphasizes that this 80-125% range is statistically derived from a 20% difference threshold, which is considered clinically insignificant for most drugs. This ensures that any variation between the generic and brand-name drug will not affect patient outcomes.
The Abbreviated New Drug Application (ANDA)
To get a generic drug approved, manufacturers submit an Abbreviated New Drug Application (ANDA) to the FDA. Unlike a New Drug Application (NDA) for brand-name drugs, an ANDA does not require new preclinical or clinical trials to prove safety and efficacy. Instead, it relies on the data already submitted for the reference listed drug.
The ANDA process typically takes 10-12 months for standard reviews. As of 2022, the first-cycle approval rate was around 65%. Common challenges include formulation issues that affect dissolution profiles and manufacturing inconsistencies that impact bioavailability. Manufacturers often need to reformulate or optimize processes based on FDA feedback during the development phase.
In recent years, the FDA has increased transparency requirements. Since 2021, ANDA applicants must submit data from all bioequivalence studies conducted on a drug product formulation, not just those demonstrating bioequivalence. This helps the agency identify potential issues early and ensures a more rigorous review process.
Narrow Therapeutic Index Drugs
While the 80-125% rule works for most medications, some drugs have a narrow therapeutic index (NTI). These are drugs where small differences in blood concentration can cause treatment failure or toxicity. Examples include warfarin (a blood thinner) and levothyroxine (used for thyroid conditions).
For NTI drugs, the FDA may recommend tighter bioequivalence limits. Although the standard 80-125% range is appropriate for most medications, experts note that extra caution is needed for NTI drugs to ensure patient safety. The FDA publishes product-specific guidances for generic drug development, with over 2,000 guidances available as of 2023, detailing the agency's current thinking on how to develop specific generic drug products.
Complex Generics and Future Directions
As pharmaceutical technology advances, so do the challenges of proving bioequivalence. Complex generics, such as topical creams, inhalers, and extended-release formulations, often require specialized testing methods. Standard bioequivalence assessment can be challenging for these products, leading the FDA to develop new guidance documents.
The FDA’s 2022-2026 strategic plan for generic drugs includes the use of modeling and simulation approaches to potentially reduce the need for clinical bioequivalence studies for certain products. This could speed up the approval process while maintaining high safety standards. Industry analysts predict continued refinement of bioequivalence standards for complex generics, with the Generic Pharmaceutical Association forecasting 20% annual growth in complex generic approvals through 2025.
Why Bioequivalence Matters for Patients
Generic drugs account for approximately 90% of prescriptions filled in the United States but only about 20% of total drug spending. Over the decade 2010-2019, generics saved the U.S. healthcare system an estimated $1.7 trillion. This cost savings is possible because the FDA’s bioequivalence requirements ensure that generics are therapeutically equivalent to brand-name drugs.
When you switch from a brand-name drug to a generic, you can trust that it will work the same way. The FDA’s rigorous standards protect patients by ensuring that any generic drug on the market has been thoroughly tested for bioequivalence. This allows doctors to prescribe generics confidently, knowing they provide the same clinical benefits as their brand-name counterparts.
What is the difference between bioequivalence and pharmaceutical equivalence?
Pharmaceutical equivalence means the generic drug contains the same active ingredient, dosage form, route of administration, and strength as the brand-name drug. Bioequivalence goes further by proving that the generic drug is absorbed into the bloodstream at the same rate and extent as the brand-name drug. Both are required for FDA approval of a generic drug.
Can generic drugs have different side effects than brand-name drugs?
Generally, no. Because bioequivalence ensures the same rate and extent of absorption, the clinical effect and potential for adverse effects should be the same. However, inactive ingredients (excipients) may differ, which could rarely cause allergic reactions in sensitive individuals. Always consult your doctor if you experience unexpected side effects.
Why does the FDA allow an 80-125% range for bioequivalence?
The 80-125% range is statistically derived to ensure that any difference between the generic and brand-name drug is clinically insignificant. It accounts for natural variability in human metabolism. The requirement that the entire 90% confidence interval falls within this range ensures a high level of certainty that the drugs are therapeutically equivalent.
Are all generic drugs tested in humans?
Most systemic drugs intended for absorption into the bloodstream are tested in humans (in vivo). However, for drugs acting locally, such as topical creams or eye drops, in vitro testing (lab-based) may be sufficient. The FDA provides specific guidances for each type of drug to determine the appropriate testing method.
What is a Narrow Therapeutic Index (NTI) drug?
An NTI drug is a medication where small changes in blood concentration can lead to serious health risks, such as toxicity or treatment failure. Examples include warfarin and levothyroxine. For these drugs, the FDA may recommend tighter bioequivalence limits to ensure patient safety, although the standard 80-125% range is still used for most medications.

