The Grading System: How Doctors Measure Aggression
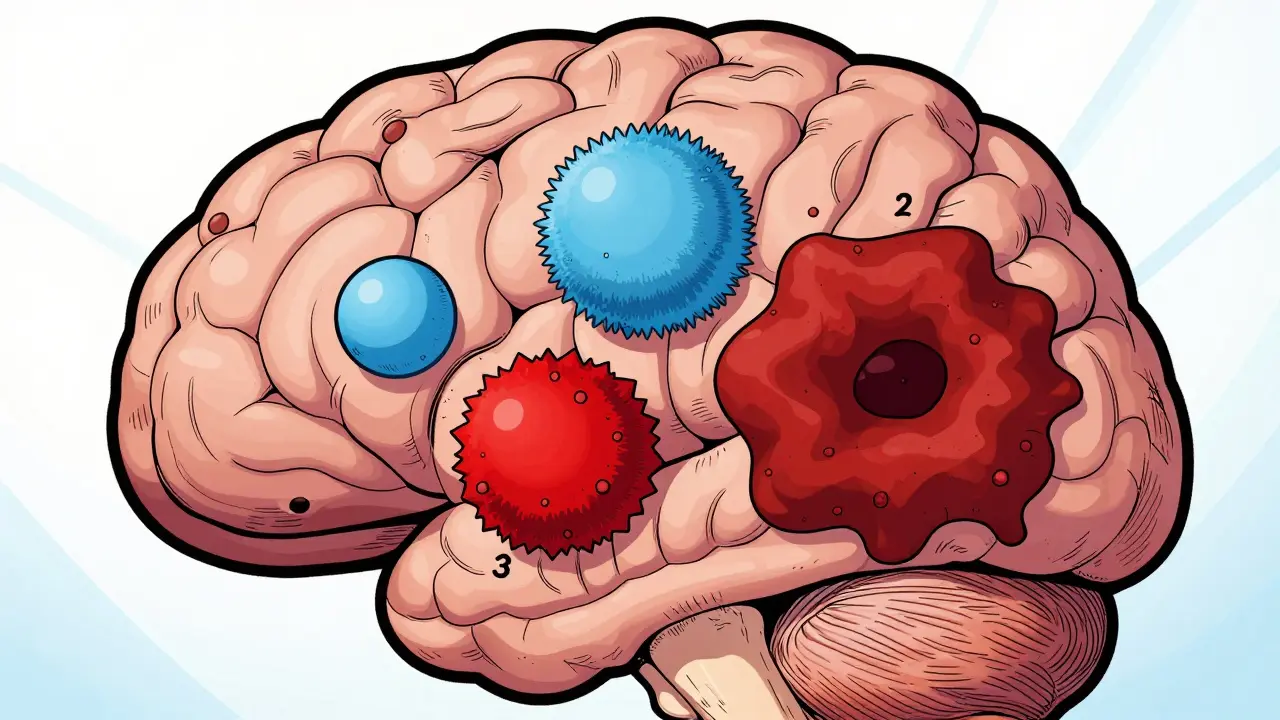
When a pathologist looks at a tumor under a microscope, they aren't just looking for the presence of cancer; they are looking at how the cells behave. The global standard for this is the WHO Classification of Tumors of the Central Nervous System, specifically the fifth edition known as WHO CNS5. Instead of just guessing how fast a tumor might grow, doctors use a grading scale from 1 to 4. It's a bit like a speed limit for cancer: the higher the number, the faster the tumor typically spreads.- Grade 1: These are low-grade tumors. They grow slowly, have clear edges, and usually stay put in one spot. They are often treatable with surgery alone.
- Grade 2: Still considered low-grade, but these cells are slightly more abnormal. They can sneak into nearby healthy tissue, which means they have a higher chance of coming back after surgery.
- Grade 3: Now we enter high-grade territory. Often called "anaplastic," these tumors are actively proliferating and aggressively invading surrounding brain tissue.
- Grade 4: The most aggressive. These tumors multiply rapidly, create their own blood vessels to feed their growth, and often have dead (necrotic) centers because they grow faster than their blood supply can keep up.
The Shift to Molecular Diagnostics
For decades, doctors relied solely on how a tumor looked under a microscope (histology). But the 2021 WHO CNS5 update changed the game by bringing in molecular markers. Think of histology as looking at the "shape" of the car, while molecular diagnostics is looking under the hood at the "engine." By identifying specific mutations, doctors can now diagnose tumors with far more accuracy. For example, the status of IDH (Isocitrate Dehydrogenase) is now a primary deciding factor. An IDH-mutant astrocytoma behaves very differently than an IDH-wildtype glioblastoma, even if they look similar under a microscope.| Tumor Type | Common WHO Grade | Key Molecular Marker | Growth Characteristics |
|---|---|---|---|
| Pilocytic Astrocytoma | 1 | BRAF mutation (common) | Slow, well-defined |
| Oligodendroglioma | 2-3 | IDH-mutant & 1p/19q-codeleted | Infiltrative, slower growth |
| Glioblastoma | 4 | IDH-wildtype | Rapid, highly invasive |
| Meningioma | 1-3 | Varies by grade | Surface-level, varies in aggression |
Multimodal Treatment: The "All-of-the-Above" Approach
Because brain tumors are so complex, a single treatment rarely does the job. Doctors use a multimodal strategy, which means combining different types of therapy to attack the tumor from multiple angles.- Surgical Resection: The goal is "maximal safe resection." Surgeons want to remove as much of the tumor as possible without damaging critical brain functions (like speech or movement). For low-grade tumors, this might be a cure. For high-grade tumors, it's usually the first step to reduce the tumor load.
- Radiation Therapy: Using high-energy beams to kill remaining cancer cells. This is often used after surgery to "mop up" microscopic cells that the surgeon couldn't see or reach.
- Chemotherapy: Drugs like Temozolomide are often used. The Stupp protocol is the standard for glioblastoma, combining chemotherapy with radiation.
- Targeted Therapy: This is the newest frontier. Drugs like vorasidenib specifically target IDH-mutant tumors. In recent clinical trials, this targeted approach significantly extended progression-free survival compared to traditional methods.
Navigating the Diagnostic Journey
Getting a final diagnosis is often the most stressful part. It usually takes about 7 to 10 business days from the time of a biopsy for the pathology report to be finalized. This is because the lab has to perform both the visual exam and the expensive molecular testing (which can cost several thousand dollars). One major hurdle is the "diagnostic gap." Many patients experience delays of several weeks before getting an answer. If you are in this process, it's helpful to know that the wait isn't just bureaucratic-it's because the molecular testing required for an accurate WHO CNS5 grade is technically demanding.
Living with the Diagnosis
Beyond the clinical side, a brain tumor diagnosis disrupts everything. For younger patients, this often means making rapid-fire decisions about things like fertility preservation before starting chemotherapy or radiation, which can permanently affect reproductive health. Support systems have evolved. The National Comprehensive Cancer Network (NCCN) provides detailed guidelines for 12 major tumor types, which helps patients and doctors stay aligned on the most current evidence-based treatments. There is also a growing movement toward "liquid biopsies," where doctors can detect tumor DNA in cerebrospinal fluid, potentially reducing the need for invasive brain biopsies in the future.What is the difference between a primary and secondary brain tumor?
A primary brain tumor starts in the brain or its tissues. A secondary (or metastatic) brain tumor starts elsewhere in the body-like the lungs or breast-and spreads to the brain. The grading and treatment strategies discussed here primarily focus on primary tumors.
Does a Grade 4 diagnosis always mean the tumor is untreatable?
No. While Grade 4 tumors like glioblastoma are aggressive, they are treatable. Outcomes vary wildly based on molecular markers. For instance, IDH-mutant grade 4 tumors generally have a much better median survival rate than IDH-wildtype versions.
How often should I have follow-up MRIs?
Follow-up schedules depend on the grade. Low-grade tumors may be monitored every 6 to 12 months, while high-grade tumors require much more frequent imaging-sometimes every 2 months-to catch any recurrence early.
What is 1p/19q-codeletion?
This is a specific genetic change where parts of chromosomes 1 and 19 are missing. It is a hallmark of oligodendrogliomas and is a positive marker because these tumors typically respond better to chemotherapy than other types of gliomas.
Can brain tumors be cured?
Some can. Many Grade 1 tumors can be completely removed via surgery, resulting in a cure. For higher grades, the goal often shifts from "cure" to "long-term management" and extending quality of life.















william wang on 19 April 2026, AT 07:19 AM
The part about the diagnostic gap is so real. Most people don't realize how much the molecular testing slows things down, but having that IDH status is absolutely critical for the treatment plan.