
When a baby develops dry, itchy patches on their cheeks or arms, it’s easy to think it’s just dry skin. But for many families, that rash is the first sign of something bigger - a chain reaction called the atopic march. It’s not a guaranteed path, but for some children, eczema sets off a sequence that leads to food allergies, hay fever, and even asthma. The good news? We now know more than ever about how this happens - and how to stop it before it starts.
What Exactly Is the Atopic March?
The atopic march used to be taught like a timeline: eczema first, then food allergies, then asthma and allergic rhinitis. It sounded inevitable. But recent studies show that’s not the whole story. Only about 3.1% of children with eczema follow that exact pattern. Most don’t. Some develop multiple conditions at once. Others never go beyond the rash. The old model is outdated.
Today, experts call it atopic multimorbidity - meaning these conditions often overlap, influence each other, and don’t always appear in order. Still, eczema remains the strongest early warning sign. About 17-24% of children worldwide get eczema before age 5. And among those kids, the risk of later allergies doesn’t come from the rash itself - it comes from what’s happening underneath the skin.
Why Skin Barrier Failure Is the Root Cause
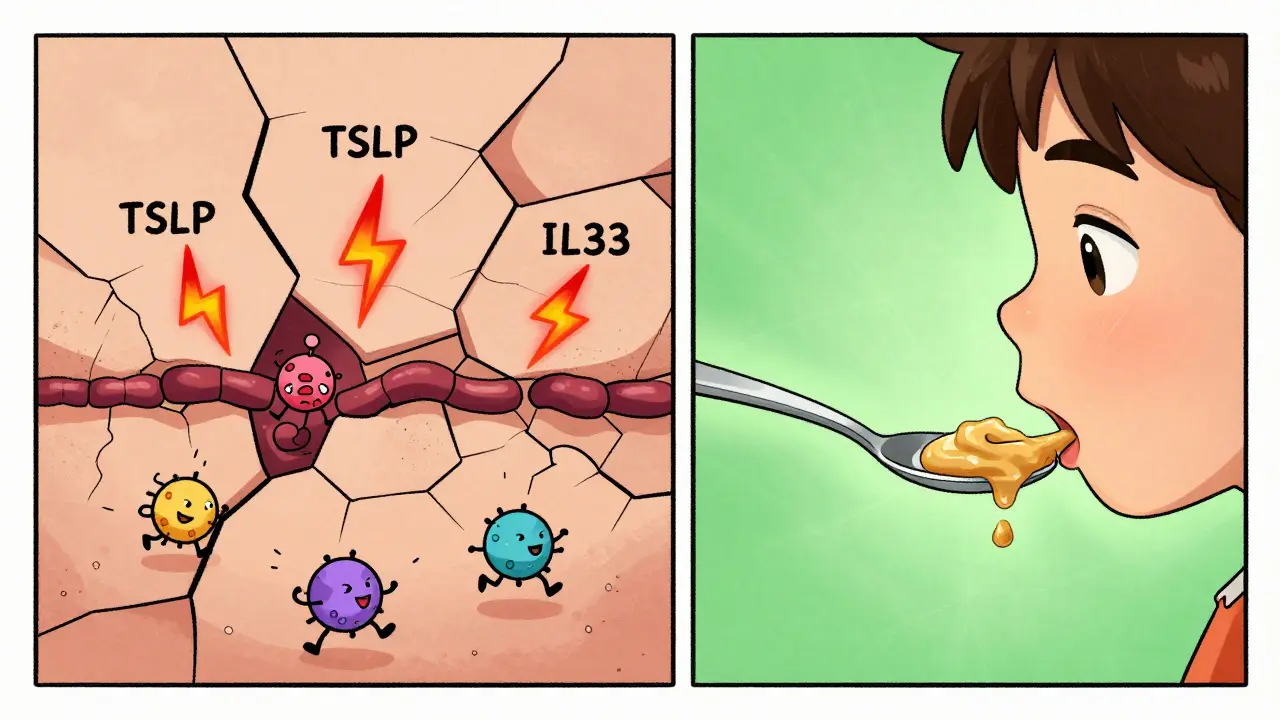
Your skin isn’t just a covering. It’s a living wall. In healthy skin, cells stick tightly together, held in place by proteins like filaggrin. This protein helps lock in moisture and keeps out dust, pollen, and food particles. But in kids who develop eczema, filaggrin is often missing or broken due to genetic mutations. These mutations aren’t rare - they’re found in up to 50% of children with moderate to severe eczema.
When filaggrin is faulty, the skin cracks. Tiny gaps open up. Suddenly, things like peanut dust, egg particles, or cow’s milk proteins can slip through. The immune system sees them as invaders. It reacts. It learns. And that’s how sensitization begins - long before the child ever eats those foods.
This isn’t just theory. The LEAP study showed that high-risk babies with severe eczema who were given peanut protein to eat early (between 4-11 months) had an 86% lower risk of developing peanut allergy by age 5. Why? Because eating peanut taught the immune system to tolerate it. But if peanut touched the skin first - through cracks - the immune system learned to attack it.
Genes Don’t Act Alone: The Role of TSLP and IL-33
It’s not just filaggrin. Other genes are involved too. Two big players are TSLP and IL-33. These are signaling proteins that act like alarms in the skin. When the barrier breaks, these genes get turned up. They tell immune cells: “Something’s wrong here.”
Children with certain variations in these genes are 1.2 to 1.8 times more likely to develop eczema, food allergies, or asthma. In fact, the same genetic changes that raise the risk of eczema also raise the risk of asthma. That’s why these conditions cluster - not because one causes the other, but because they share the same broken foundation.
And it’s not just the skin. The gut plays a role too. Studies from the BAMSE cohort and others show that babies who develop multiple allergies often have different gut bacteria. Specifically, they lack microbes that produce butyrate, a short-chain fatty acid that helps calm the immune system. Babies with low butyrate potential are more likely to become sensitized to food and airborne allergens.
How Severe Is the Eczema? That’s the Key
Not all eczema is the same. Mild flares on the arms? The risk of future asthma is low. But severe, widespread eczema that starts before 3 months? That’s a red flag.
Research from the MAS cohort study found that children with severe eczema have 3-4 times higher risk of developing multiple allergic conditions. The TOACS study showed that while 80% of kids with eczema become sensitized to allergens (meaning their immune system reacts to them), only about 25% actually develop clinical symptoms like asthma or allergic rhinitis.
Here’s the critical takeaway: Sensitization is not the same as allergy. A child can test positive for egg allergy on a skin prick test but eat eggs without a problem. That’s sensitization. True allergy means symptoms - hives, vomiting, wheezing. Only the latter requires avoidance. So don’t panic if a test is positive. Look at what’s happening in real life.
Protecting the Skin Barrier: What Actually Works
If the barrier is the problem, fixing it should help - and evidence says it does.
The PreventADALL trial gave daily emollients (fragrance-free moisturizers) to newborns at high risk for eczema. By age 1, those babies had 20-30% fewer cases of eczema than those who didn’t use moisturizer. That’s not a small win. It’s a prevention strategy.
What kind of moisturizer? Look for these:
- Thick creams or ointments (not lotions)
- Free of fragrance, dyes, and harsh preservatives
- Contains ceramides, cholesterol, or fatty acids - ingredients that rebuild the skin barrier
Apply it at least once a day - ideally right after a bath while skin is still damp. Don’t wait until the skin cracks. Start early. Even if your baby doesn’t have eczema yet, if there’s a family history of allergies, this is one of the few proven ways to lower risk.
And yes - bathing is fine. In fact, daily lukewarm baths (5-10 minutes) help remove irritants. Just follow up immediately with moisturizer. No soap unless needed. Use a gentle cleanser only on dirty areas.
Early Food Introduction: The Other Half of the Strategy
Moisturizing protects the skin. But what about what goes in the mouth? The LEAP study wasn’t a fluke. Multiple studies now confirm: introducing common allergens early - especially in high-risk babies - reduces allergy risk.
Start with:
- Peanut (thinned with water or mixed into puree - never whole nuts)
- Egg (well-cooked, scrambled or hard-boiled)
- Milk (in small amounts as part of cooked foods, like pancakes or yogurt)
Introduce one at a time. Wait 3-5 days between new foods. Watch for reactions - rash, vomiting, swelling. If there’s a reaction, stop and talk to your doctor. But if nothing happens? Keep offering it regularly. Consistency matters more than one-time exposure.
Don’t wait until 12 months. Start between 4-6 months, once your baby is ready for solids. And if your child already has severe eczema? Talk to your pediatrician or allergist before starting. They may recommend testing first.

What Doesn’t Work - And Why
There’s a lot of noise out there. Let’s cut through it.
- Organic diets? No strong evidence they prevent allergies.
- Probiotics? Some studies show tiny benefits, but results are mixed. Not recommended as a standalone strategy.
- Delaying allergens? That’s the old advice - and it made things worse. Delaying peanut, egg, or milk increases risk.
- Special hypoallergenic formulas? Only needed if a baby is allergic to cow’s milk protein. Not helpful for prevention in healthy babies.
Stick to the science: repair the skin, introduce foods early. That’s it.
When to See a Doctor
You don’t need to panic over every patch of dry skin. But if your child has:
- Eczema that starts before 3 months
- Rash covering large areas (face, arms, legs)
- Constant itching that disrupts sleep
- A family history of asthma, hay fever, or food allergies
Then it’s time to talk to your pediatrician or a dermatologist. They can help you assess risk, recommend moisturizers, and guide safe food introduction.
And if your child already has food allergies? Don’t avoid them completely. Work with an allergist. Many kids outgrow milk and egg allergies by age 5. Testing and supervised challenges can help determine if tolerance has developed.
The Bigger Picture: Precision, Not Prediction
We’re moving away from one-size-fits-all advice. Not every child with eczema will develop asthma. Not every child with a family history will get allergies. But we can now identify the ones who are most at risk - using genetics, severity of eczema, gut health markers, and early exposure patterns.
The goal isn’t to prevent all allergies. It’s to prevent the ones that matter - the ones that lead to chronic illness, hospital visits, or lifelong restrictions. And that starts with the skin.
Think of it this way: the skin barrier is the first line of defense. When it fails, the immune system gets confused. But when we help it heal - before allergens get through - we give the body a chance to stay calm.
This isn’t about perfection. It’s about consistency. Daily moisturizer. Early food introduction. No guesswork. Just science.
Can eczema cause food allergies?
Eczema itself doesn’t cause food allergies. But when the skin barrier is broken - especially in babies with filaggrin mutations - allergens like peanut or egg can enter through cracks in the skin. This can trigger the immune system to react, leading to sensitization. If the child later eats the same food, the immune system may overreact, causing a true food allergy. That’s why protecting the skin and introducing foods orally early is so important.
Is the atopic march still a valid concept?
Yes, but not as a strict sequence. The old idea that eczema always leads to asthma is outdated. Only about 3.1% of children with eczema follow that exact path. Today, experts use the term "atopic multimorbidity" - meaning these conditions often overlap, happen at the same time, or appear in different orders. Eczema is still the strongest early warning sign, but it doesn’t guarantee what comes next.
Do I need to use special moisturizers for my baby?
You don’t need expensive or branded products. Look for thick creams or ointments (not lotions) that are fragrance-free and contain ceramides, cholesterol, or fatty acids. These ingredients help repair the skin barrier. Simple options like petroleum jelly (Vaseline) or generic ceramide creams work well. Apply once daily, right after a bath, to lock in moisture.
Should I delay introducing peanut or egg to my baby?
No - unless your baby has severe eczema or a known food allergy. For most babies, introduce peanut and egg between 4 and 6 months, once they’re ready for solids. Start with small amounts: a teaspoon of peanut butter thinned with water, or a small piece of well-cooked egg. Offer it regularly (2-3 times a week). The LEAP study showed this reduces peanut allergy risk by 86% in high-risk infants.
Can gut health affect my child’s risk of allergies?
Yes. Research shows that babies who develop multiple allergies often have different gut bacteria - especially lower levels of microbes that produce butyrate, a compound that helps calm the immune system. While probiotics aren’t a guaranteed fix, breastfeeding, a varied diet after 6 months, and avoiding unnecessary antibiotics can support healthy gut development. This may help reduce allergy risk over time.







Melissa Starks on 19 March 2026, AT 21:13 PM
Okay but let’s be real - this whole 'repair the skin barrier' thing feels like corporate wellness propaganda wrapped in science jargon. I’ve been using Vaseline on my kid since day one, no fancy ceramides, no 'clinical-grade' nonsense. He’s 3, no allergies, no asthma, and we never once bought one of those $40 'eczema-specific' creams. The real problem? Over-sanitizing everything. Kids need dirt. Microbes. Exposure. You think wiping their skin with sterile ointments every day is helping? Nah. It’s making them fragile. Let them play in the yard. Let them lick the floor. Their immune system isn’t broken - it’s just bored.
Also, 'early food introduction'? My grandma fed my mom peanut butter on toast at 6 months. No studies. No trials. Just food. And we’re all fine. Why are we turning parenting into a lab experiment?